Sialendoscopy-Salivary Gland Endoscopy
Sialendoscopy – Salivary Gland Endoscopy – Dr Atilla Şengör
Sialendoscopy means ‘endoscopy of the salivary gland’. We perform this diagnostic procedure in patients who experience recurrent swelling of the salivary glands. This is how we look inside the salivary ducts to find the cause of the blockage. As in many other specialities, we also use an endoscope here. This allows us to evaluate the major salivary glands under the chin (submandibular) and in the cheek (parotid glands). Various diseases can occur in the ducts of these glands. Salivary gland stones, duct strictures (stenosis) and secretion condensation (mucus plugs) are the most common ones. Foreign bodies, duct polyps (reactive tissue formations) and inflammatory diseases may also be present. When these block the duct, saliva cannot flow and the gland may become swollen; the swelling can happen again. Sialendoscopy allows us to identify the obstructive disease directly.
We do not use this method for salivary gland tumours or minor salivary glands. These are not related to the ductal system. The endoscopes used for salivary gland endoscopy are much thinner than other standard endoscopes. These endoscopes have three channels; optical channel, irrigation and working channel. The outer diameters of the sialendoscopes used by Dr Atilla Şengör are 1.1 mm and 1.6 mm. They are instruments almost as thin as a toothpick. Their working channels are 0.4 or 0.8 mm. The necessary treatment for a stone or stenosis is performed through these working channels with very thin instruments. For this reason, the costs in sialendoscopy are high.
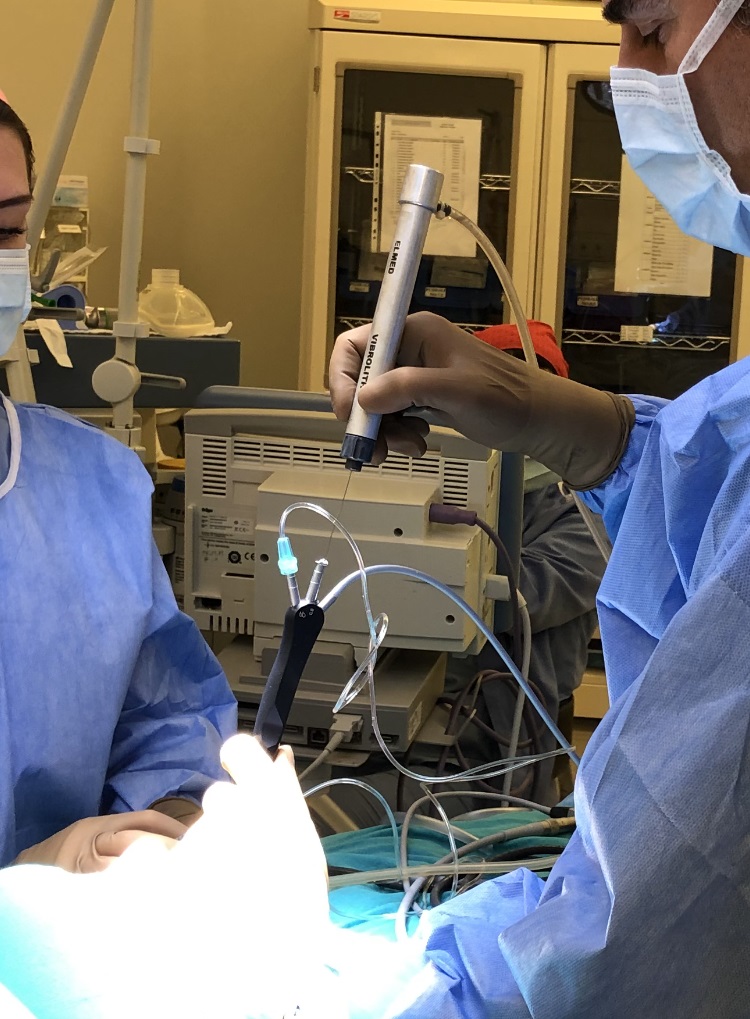
Sialendoscopy is a relatively short procedure that we prefer to perform under sterile condition. We prefer to perform this in an operating theatre. Sialendoscopy can be done under local anaesthesia. However, if we encounter a stone, it is better to anaesthetise the patient, as removing it can take a long time. We prefer general anaesthesia in such cases so the patient remains comfortable and does not experience distress. Procedures such as stone removal, fragmentation, ductal dilatation, and stenting can be performed during sialendoscopy. We refer to these as ‘interventional sialendoscopy
Sialendoscopic diagnosis and treatment began to be used worldwide in the 1990s. Dr. Atilla Şengör started working in this field in 2004 and is the pioneer of this method in Türkiye. He developed the technique of fragmenting stones within the duct (pneumatic lithotripsy). He has published both national and international articles and continues to give lectures at conferences. In 2008, he is one of the authors of the first Turkish book on this subject. You can see some of his works in the ‘Selected Publications’ section. You can see the conferences he attended/spoke at in his biography. With the advent of sialendoscopy, the approach to diagnosing and treating salivary gland duct diseases has changed. In particular, open surgeries for salivary gland stones have decreased worldwide.
Is sialendoscopy an operation?
Sialendoscopy is actually a diagnostic method. We use it to look inside the ducts of the salivary glands. Today, endoscopes are used to view many parts of the body by illuminating and magnifying them, and they also allow us to record images. The endoscopes used in the salivary gland ducts are called “sialendoscopes.” The instruments used in sialendoscopy are very thin and delicate. Sometimes, the help of an assistant and anaesthesia may be required. Therefore, we prefer to perform sialendoscopy in an operating theatre.
Interventions performed during sialendoscopy can be considered surgical, but they are minimally invasive procedures. We perform procedures such as salivary gland stone removal or stenosis dilatation by working inside the duct. We only treat the obstruction; the salivary gland itself is not removed. Therefore, risks associated with open surgery, such as scarring, facial paralysis, or vascular injury, are avoided in sialendoscopy.
What Are Salivary Glands? Anatomy, Function, and Sialendoscopy
Salivary glands are organs that produce saliva. Saliva keeps the mouth moist and helps lubricate food while chewing. It also plays an important role in swallowing and digesting food. The large salivary glands are called “major salivary glands.” They have a duct system. The major salivary glands are located on the cheek (parotid gland), under the chin (submandibular gland), and beneath the tongue (sublingual gland). The saliva produced by these glands flows into the mouth through their main ducts. The openings of these ducts, where they drain into the mouth, are located under the tongue or inside the cheek. We can access the salivary ducts using sialendoscopy. If a disease is blocking the duct, we can both diagnose and treat it.
There are also hundreds of small salivary glands in the mouth, called “minor salivary glands.” When you touch your tongue to the inside of your lips, the small bumps you feel are these glands. However, sialendoscopy cannot be performed on them because they are too small. In cases where Sjögren’s syndrome is suspected, a few of them can be removed for pathological examination.
Understanding Salivary Gland Ducts: Anatomy, Function, and Stones?

Anatomical segmentation of the salivary duct system as seen during sialendoscopy.
The salivary gland and ducts can be compared to a tree. We can think of the leafy part as the part where saliva is produced (parenchyma). Thin ducts originating from the parenchyma continue to thicken towards the trunk, just like the branches of a tree. The ducts coming from different parts of the gland merge to form the main duct (trunk). The diameter of the branches/ducts in this system varies between 0.5mm and 3.2 mm. The main duct carries saliva towards the mouth and drains it through the points we call orifices. The orifices, which are as thin as the tip of a needle, are located in the papillae. These are the bumps on the inside of the cheeks and under the tongue. Even very small stones can be caught in these funnel-shaped areas. When saliva is blocked, the gland swells. During sialendoscopy, we first enlarge this orphis and then enter the duct. We proceed in the canal system as far as the diameter of the canal allows. This distance varies between 5 and 9 cm.
As I mentioned above, the duct system is like a tree; the branches continue into the gland. Therefore, there is no such distinction as ‘inside the gland’ or ‘in the duct’ for a stone in endoscopy. These expressions are often used erroneously by those who do not perform sialendoscopy or have poor knowledge of anatomy. When we enter the duct with a sialendoscope, we can reach 80-85% of the stones regardless of the duct-gland distinction. Anyway, stones are usually in the main duct or thick branches. Problems in the thin and end branches do not cause swelling of the entire gland and do not cause significant complaints.
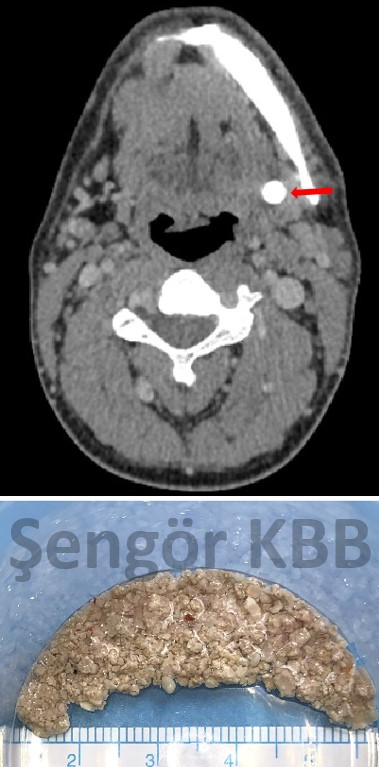
Left submandibular salivary stone (1 cm in diameter, intraglandular) on CT and the collected fragments after sialendoscopic intraductal fragmentation.
Do All Salivary Gland Swellings Mean a Stone?
Salivary gland stones are the most common cause of salivary gland swelling. They usually cause swelling under the chin or in the cheek. Stenosis, which was briefly mentioned above, is the second most common cause. Part of the duct or sometimes the entire duct may become narrowed. In some cases, stenosis occurs only at the duct opening (orifice). Intraoral incisions without sialendoscopy often cause this type of stenosis. When saliva cannot pass through the stenotic area, the gland swells.
Swelling may be caused by autoimmune diseases like Sjögren’s or radioactive iodine therapy. Radiation sialadenitis occurs in patients treated with radioiodine for thyroid cancer. Juvenile recurrent parotitis causes repeated inflammation of the parotid gland in childhood. In these cases, the secretory cells are mainly affected, and duct stenosis may occur. We can help these patients by widening the salivary gland ducts using sialendoscopy.
Other duct conditions, like mucus plugs, duct polyps, and foreign bodies, can cause swelling. Not all salivary gland swellings are caused by duct obstruction. Everyone has heard of mumps, which mostly affects children. In mumps, the secretory cells of the parotid (cheek) gland become inflamed and swollen. Sometimes, masses in the gland appear as swelling and gradually grow. These can be benign or malignant tumors. Sialendoscopic procedures are not used for mumps or tumors.
The most common symptom of all these conditions is swelling of the affected gland. In these cases, we evaluate the duration of symptoms and clinical findings. For example, in patients with salivary gland stones or duct stenosis, swelling usually occurs during meals.
Salivation is stimulated by eating, by sour flavors, or even by smell. If the salivary duct is obstructed, saliva cannot drain and the gland swells. When the obstruction is partial, the swelling gradually subsides. If the stone grows, the blockage worsens and the gland takes longer to shrink. If the duct is completely blocked, the gland may remain permanently swollen.
Depending on the clinic, preliminary diagnoses are made using tests and imaging methods.
Is Sialendoscopy a New Technique? Is it available in every hospital?
Sialendoscopy can no longer be considered a new technique. It was first applied worldwide in the 1990s. In 2007, we developed the pneumatic stone fragmentation method in the duct. In 2008, we published the first book on this subject in our country. We introduced our fragmentation method internationally at the 1st International Sialendoscopy Congress in Geneva in 2012. Since then, the method has progressed significantly, and German colleagues have also started using this technique.
Therefore, as of 2025, we have been working on sialendoscopy in our country for 21 years. During this time, we have promoted the method among colleagues through publications and presentations. We also inform patients via articles and posts so they can understand, request, and benefit from this technique.
Unfortunately, the devices and tools used for sialendoscopy are not available in most hospitals. These instruments are very delicate and expensive, and the sialendoscopy method requires advanced endoscopic experience. When tools break, practitioners often cannot finance replacements and, unfortunately, cannot continue performing the procedure.
Fortunately, education in sialendoscopy is now available locally. It is being applied in several centres. However, sialendoscopy tools remain scarce in many hospitals. Availability alone does not ensure that every specialist can use them. The sialendoscopist must have adapted the stone fragmentation devices to the procedure in their practice.
In salivary gland stone treatment, we use intraductal fragmenting and combined approaches. This raised our success rate from 40% to over 90%.
Are any incisions made during sialendoscopy?
In most cases, sialendoscopy is performed without any incision. We gently widen the salivary duct opening with thin dilators and advance the sialendoscope. Stones are fragmented inside the duct and removed either by washing or using fine instruments. Under normal conditions, no incision is required.
Sometimes, however, a small incision becomes necessary. If the duct opening is too narrow, a controlled cut called papillotomy can be made. This helps us enter the duct safely and also prevents future narrowing.
In some stone cases, there may not be enough space to perform sialendoscopy. If stones are near the duct opening under the tongue or cheek, a small incision may be needed. This procedure is known as salivary gland stone surgery. Incisions performed without sialendoscopy can damage the duct and cause it to close, limiting future treatment options.
If surgery is unavoidable, we use a sialendoscopy-guided approach. First, the stone is located inside the duct. The incision is made directly over the stone, which is then removed. Afterwards, the duct is re-examined with the sialendoscope to ensure no stones remain. At the end, the duct is repaired with ductoplasty and supported with a stent.

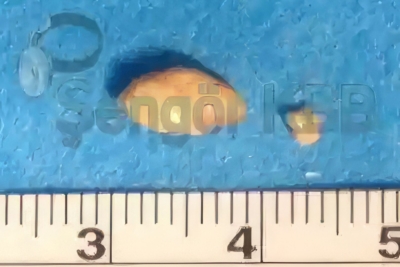
A submandibular stone removed in one piece via sialodochotomy
Can large stones be removed with sialendoscopy?
In many cases, large or giant salivary gland stones can be removed using sialendoscopy combined with crushing (fragmenting) methods. With experience, stone size mainly affects working time, not success. Stones can be broken with pneumatic lithotripsy (air pressure) or Holmium laser. Pneumatic lithotripsy allows long procedures without heat damage, which is a key factor in achieving high success rates. During sialendoscopy, the crushing (fragmenting) probe must touch the stone to break it. If a stone is embedded or the duct does not allow access, it cannot be reached or seen with the sialendoscope. Unseen stones cannot be broken in this way.
About 80–85% of stones can usually be reached with the sialendoscope, and our success rate for reachable stones is 94% over 20 years. These success rates are similar for both small and large stones.
Is hospitalisation necessary after sialendoscopy?
Sialendoscopy is a minimally invasive endoscopic procedure and not a major surgery. Patients can usually be discharged on the same day. The procedure is generally performed under anaesthesia, which requires a hospital setting. Anaesthesia effects may last several hours, so patients typically rest for about five hours after waking up. In rare cases with prolonged anaesthesia, overnight hospitalisation may be needed. Patients coming from out of town or abroad may also stay overnight for convenience, and they are discharged the next day.
Some patients may have multiple salivary gland stones
What is the treatment process after sialendoscopy?
During sialendoscopy, irrigation fluid is continuously introduced into the salivary duct. After the procedure, some swelling in the gland is common and may last from a few hours to a few days. Mild pain from swelling may occur for 1–2 hours, and paracetamol-type painkillers are usually sufficient. A stent is usually placed in the duct, which can slightly slow saliva flow. Drinking fluids and gently massaging the gland can help reduce swelling.
When the stone is removed, healing begins immediately. After stent removal, swelling during meals disappears. Over time, saliva flow and taste improve. In cases with long-standing problems, it may take months for the gland to fully return to normal, and rarely, some swelling may persist. This should not be confused with age-related salivary sagging.
Because the procedure is performed through the mouth, antibiotics are given for 5 days during and after the operation to prevent infection. In rare cases, the stent may need to stay in place for 2–3 weeks. The thin plastic stent is easily removed in the office without discomfort, like removing a stitch.
How are the controls after sialendoscopy?
After sialendoscopy, patients are checked at specific intervals. The stent is usually removed after one week. It is helpful to evaluate the duct function and the consistency of saliva at the 2nd week and 1st month. For patients coming from outside Istanbul, we try to adapt these follow-ups conveniently.
In some cases, stones cannot be totally removed or reached with sialendoscopy, which occurs in about 15–20% of patients. Occasionally, some stones or fragments may remain. These patients need long-term follow-up for swelling attacks and gland inflammation. During sialendoscopy, the duct is widened. This allows some stones to move with saliva flow and even fall out spontaneously over months or years. Sometimes, stones move closer to a position suitable for removal. In such cases, a second sialendoscopic procedure may be helpful. If symptoms worsen and cannot be tolerated, surgical removal of the gland may be considered.
How long does it take to return to daily life after sialendoscopy?
Sialendoscopy is generally not tiring for the patient. If only diagnostic sialendoscopy is performed under local anaesthesia, patients can return to normal activities the same day. Procedures to fragment salivary gland stones under general anaesthesia may take longer. In such cases, patients should rest for 1–2 days before resuming normal activities.
Do private insurances cover sialendoscopy?
Private insurance policies are agreements between the insurer and the patient. Coverage depends on the disease onset and policy date. Most private health insurances may cover sialendoscopy. We communicate with international patients beforehand, collect the necessary documents, and help complete the insurance forms.
The treatment fee is calculated based on standard medical units, experience level, and device usage. The final fee may vary depending on the number and size of stones. For example, small stones may reduce the fee, while large stones in one or both glands may increase it. After reviewing the patient’s imaging, we calculate the fee and inform the patient in advance. The fee is fixed in Turkish Lira and can be converted to the patient’s local currency if needed.