Salivary Gland Stone Treatment
 Today, salivary gland stone treatment, medically known as “sialolithiasis treatment”, is performed inside the duct of the salivary gland using thin endoscopes. We call this method “sialendoscopy”, in which we can hold the stones with thin instruments and remove them directly or by breaking them if necessary. We started to work on sialendoscopy in 2004 in our country, the first studies of which were brought to the agenda by German colleagues in 1990. We have done and continue to do all the pioneering work to spread it throughout the country. We owe the production of sialendoscopes to the developing medical and optical technology.
Today, salivary gland stone treatment, medically known as “sialolithiasis treatment”, is performed inside the duct of the salivary gland using thin endoscopes. We call this method “sialendoscopy”, in which we can hold the stones with thin instruments and remove them directly or by breaking them if necessary. We started to work on sialendoscopy in 2004 in our country, the first studies of which were brought to the agenda by German colleagues in 1990. We have done and continue to do all the pioneering work to spread it throughout the country. We owe the production of sialendoscopes to the developing medical and optical technology.
In the treatment of salivary gland stones, it is still recommended to remove the gland. However, in the sialendoscopy method, we remove only the stones without removing the salivary gland. In this way, we also protect the patient’s saliva secretion and functions. Our success rate in the treatment of salivary gland stones is around 80%. During sialendoscopy, we can directly remove the small stones we see with tools such as forceps and basket. For large stones that are stuck in the duct, we first break them and then remove them in pieces.
The only condition for these methods to be successful is that the stone must be reached within the canal. The rate of this is around 80-85 per cent. The probability of removing a salivary gland stone that we can reach is 94%. We achieve this thanks to the crushing method we have been using since 2007. Experience in sialendoscopy, equipment and meticulous work are also very important. Failed cases are usually due to the stone not being accessible sialendoscopically. The duct system may be too narrow or tortuous; it may not always allow the sialendoscope to advance. Sometimes salivary gland stones are too hard or embedded to be crushed. In these cases, sialendoscopy may not be helpful. However, we can simultaneously perform applications that widen and shorten the salivary duct. These can increase the likelihood of the patient dropping the stone. Sialendoscopy is an advanced technological diagnosis and treatment method. In at least 75% of cases, we need stone crushing (pneumatic lithotripsy or laser) methods. These devices must be included in the equipment and adapted for sialendoscopic use. When sialendoscopy is performed by specially trained and experienced specialists, successful results are possible.

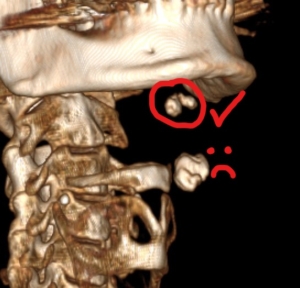
One Piece Salivary Gland Stone
What is salivary gland stone?
Just as there are stones in the kidney and gall bladder, there may also be stones in the salivary glands. These are called “salivary gland stones”. In medicine, we refer to them with the terms “sialolithiasis”, “sialolithiasis” or “calculi”. They are usually calcium-containing structures and can block the salivary ducts. They can form in conditions and diseases that inhibit saliva secretion, concentrate it and disturb its chemistry. Salivary gland stones can be single or multiple and grow over time. Depending on the gland in which they are located, the most obvious symptom is swelling in the cheek (parotid gland) or under the chin (submandibular gland). Initially, these swellings usually occur when eating; after a short time the swelling subsides.
Over time, the swelling can become permanent and inflammation/complications can occur in the gland. Salivary gland stones can be as small as 2-3 millimetres and as large as 5-6 centimetres. We know that these stones grow about 1 mm per year on average. As the stones grow, they can adhere to or become embedded in the wall of the salivary duct. Therefore, when a stone is detected, we recommend removing it by sialendoscopy. This is because the treatment of patients who wait for years may become more difficult, and even the possibility of removing the stone without surgery may decrease.
Tomography Image of Salivary Gland Stone
What causes salivary gland stones?
The question “Why does salivary gland stone occur?” can be answered within the framework of three different views:
1. A micro-sized stone forms in the secretion-producing cells of the salivary gland. This particle falls into the duct and calcium layers form around it; it grows over time.
2. The saliva secretion has a thick consistency (mucus plug). Precipitates form on the mucus plug and a stone is formed by stratification. In both of these cases, there is a nucleus originating from the duct or gland itself.
3. Some substances in the mouth can enter the salivary gland duct. These can cause stone formation. These can be organic substances, bacteria and nutrients. Of course, in all three cases, a slowed and concentrated flow of saliva can accelerate the formation of salivary gland stones. This is why we recommend that these patients drink plenty of water as part of the treatment of salivary gland stones. We know that sialolithiasis grows by an average of 1 millimetre per year.
Among the common features that we frequently see in patients with sialolithiasis, we can count the following:
– Low fluid intake, smoking and a diet poor in vegetables can trigger salivary gland stone formation.
– Smoking. Smoking reduces and intensifies saliva secretion.
– Meat-heavy diet. Phytates in cereals and grains prevent crystallisation. Salivary gland stone formation may be facilitated in people with a diet poor in vegetables.
– Use of allergy medication and some psychiatric drugs. We know that these also intensify saliva secretion. Unlike kidney stones, salivary gland stones are not related to serum calcium and phosphate levels. The only systemic disease known to cause sialolithiasis is gout.
What are the Symptoms of Salivary Gland Stone?
The most visible symptom of salivary gland stones is swelling. During or after eating, swelling occurs on the cheek, under the ear or under the chin. The swelling is due to blocked saliva flow. The accumulated saliva swells the salivary gland on the cheek or under the chin. If the duct is not completely blocked and saliva can leak from the edge of the stone, the gland goes down after a while. However, stones grow 1 mm per year. Over the years, the duct may become completely blocked and the swelling of the gland may become permanent. Swelling of the salivary gland may sometimes be accompanied by inflammation. In this inflammatory picture, which we call “acute sialadenitis” in medicine, the patient is usually treated by an ENT Specialist. As a result of the examinations, salivary gland stones may be detected in some patients.
Other symptoms of salivary gland stones include the following:
– Feeling of tension on the cheek or under the chin
– Glare in these areas
– Swelling, whiteness or redness in the mouth of the salivary duct
– Intense gel-like, greyish or inflamed secretion
– Feeling of the stone under the tongue or cheek, stinging
– Rarely dry mouth

Cheek Salivary Gland Swelling
What is good for salivary gland swelling?
A patient with a swollen salivary gland notices it on the neck or cheek. However, there may be other diseases in those areas. In order to make a preliminary diagnosis, it is best for the patient to see a doctor in the first stage. This can be a family doctor or an ENT specialist. An examination is carried out, and depending on the duration of the swelling or the presence of pain, treatment can be prescribed or investigations can be carried out.
New onset of painful swelling may be due to salivary gland inflammation, and short-term swelling that occurs while eating may be due to salivary gland stones. These swellings may last longer over time; swelling may be permanent. In masses that grow slowly over time, we consider the possibility of a tumour. Accordingly, diagnostic imaging methods are performed. We can diagnose and treat diseases that block the duct such as salivary gland stones with sialendoscopy. Therefore, the best thing for swelling of the salivary gland is to diagnose the cause. In this way, what is good for the swelling can be determined.
Salivary Gland Stone Removal Methods
In the past, drinking plenty of water was recommended as a method to reduce salivary gland stones. It was especially recommended to consume sour foods (lemon, etc.) and to massage the gland frequently. However, there was no specific time limit for these. It was offered as an option to patients who did not accept open surgery immediately. When the patient did not pass stones for years and his/her problems increased, the gland was removed by surgery. We know that stones grow up to 1 mm per year.
Therefore, the diameter of a stone can show how many years it has not dropped. In addition, inflammation while waiting can be severe and dangerous. Now that we have sialendoscopy, we do not recommend waiting for a stone to fall out. Saliva flow is already impaired in glands with stones. Painful swelling that occurs when eating and drinking sour food may cause distress to the patient. Perhaps in a severe inflammation, the stone can be dropped during the discharge of the abscess from the neck or cheek skin. However, rupture of the duct and damage to the surrounding tissues during this process is not good. This may cause narrowing or complete closure of the canal. We started to use the sialendoscopy method in our country in 2004. Since the success rate is high, we do not recommend waiting for stone dropping except for small stones near the mouth of the duct.
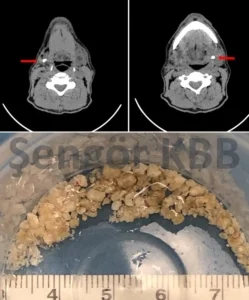
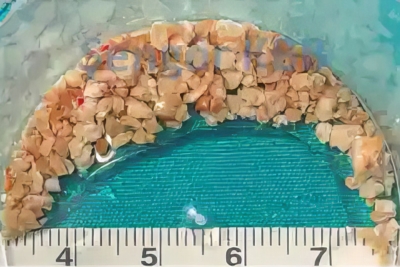
Bilateral submandibular gland salivary calculi
Salivary Gland Stone Surgery
“Salivary gland surgery” refers to the complete removal of the salivary gland. “Salivary gland stone surgery” is an attempt to remove the stone through incisions made in the mouth. The incisions made just above the stone are called sialolithotomy; duct incisions are called sialodocotomy. In the past, when there was no sialendoscopy method, palpable stones were tried to be removed with these incisions. The stones that were not palpable were expected to fall spontaneously. When the stone grew and the inflammation became severe and the patient could no longer tolerate it, removal of the salivary gland was considered.
Today, we prefer sialendoscopy at every stage of salivary gland stone treatment. With sialendoscopy, we aim to remove the stone without making any incision and without damaging the salivary gland and duct. In this way, we want saliva secretion and functions to continue. However, salivary gland stone surgery may be necessary for stones of appropriate location and size. We always perform such interventions under the guidance of sialendoscopy. Because there may be other stones deep in the duct or in the gland. In order to prevent these from being left behind, they should be examined with a sialendoscope and removed if any. We also use the sialendoscopy method during the repair of the intraoral incisions and the control of the secretion flow. In this way, we prevent the negativities that may occur after salivary gland stone surgery. I will include these in the heading below.
Risks of salivary gland stone surgery
Salivary gland stone surgery, i.e. sialodocotomy or sialolithotomy, has some risks. When this procedure is performed alone, i.e. not accompanied by sialendoscopy, some risks increase. The first of these is bleeding. Since the oral mucosa has a high blood circulation, bleeding is expected. If it is very severe, it will be difficult to continue the operation. The larger the incision, the more likely it is that the vessels and nerves will be affected. Inflammation can develop from this incision site. There are already many germs in the mouth; antibiotics are needed to suppress them. There may be pain at the incision site; painkillers may be needed. We usually do not need an incision during sialendoscopy; we can limit the incision if necessary.
The incisions made on the stone necessarily involve the salivary duct. If sialendoscopy and stenting are not performed at this stage, the duct may subsequently close or narrow. In addition, the stone may move during the incision and may escape backwards in the duct system. Even if the incised stone is removed, there may be other stones in the canal. In both of these cases, if the sialendoscope is not used, the stone will remain behind. In this way, the patient’s problem will not be solved and complaints will continue. When patients who have been intervened in this way apply later, we try to remove the remaining stones with a sialendoscope. If stenosis has developed, we try to widen it again sialendoscopically. However, if the canal is severely damaged or completely closed, these patients unfortunately lose the chance of treatment with sialendoscopy. Finally, other small salivary glands may be damaged in the incision area. These can lead to the development of retention cysts called “ranula”. This may require various surgeries afterwards.
Salivary Gland Stone Treatment with Sialendoscopy
The duration of salivary gland stone treatment with a sialendoscope depends on the number, location and size of the stones. Examinations and methods such as ultrasonography and tomography can give a preliminary idea about them. However, none of them show the condition inside the duct. Since sialendoscopic intervention starts with the visualisation of the stones, the actual treatment time is also determined at this stage.
Small stones of 2-3 millimetres in diameter, which do not exceed the diameter of the duct, can be removed directly. During sialendoscopy, they can be removed with forceps or a basket. The removal of these stones can take seconds to minutes. However, there may also be small stones that are trapped in the fine branching of the gland. For these and larger stones, crushing may be necessary. This takes at least 30 minutes and sometimes even hours.
Most large stones that are located deep in the salivary duct or inside the gland have to be crushed and removed. This requires advanced endoscopic experience and determination. Regardless of the size, if a salivary gland stone can be reached in the duct, crushing can be performed. This makes it possible to remove even very large stones up to 2.5-3 centimetres in size. Since we remove them in small pieces, it can take 2 to 5 hours. Stone crushing is necessary in at least 75 per cent of cases with salivary gland stones. Sialendoscopy can also be performed in conjunction with intraoral interventions for stones close to the duct or surface. In suitable salivary gland stones, this combination can remove the stone within 1-1.5 hours, even if it is large.
Click for detailed information about Sialendoscopy-Salivary Gland Endoscopy
Is it possible to get 100% result with sialendoscopy?
The sialendoscopy method we use for salivary gland stone treatment is a very delicate work. The salivary gland duct is 2-2,5mm in diameter. The sialendoscopes we use are 1.1mm and 1.6mm in diameter. We pass them through the 0.8mm working channel, break the stones with 0.6mm crushers and remove them with 0.8mm forceps. We can liken this work to working with a needle through a toothpick. It requires experience, skill and determination in endoscopic matters.
Another condition is the structure of the duct system. Salivary gland ducts become thinner by branching into the gland. Therefore, stones located in the end branches of the gland or embedded in the duct may not be accessible. The sialendoscope cannot enter a duct that is thinner than its own diameter. Since it is semi-flexible, it cannot progress in ducts with sharp angulation. If the stone is fully embedded in the tissue, i.e. outside the canal system, it cannot technically reach it. In the light of this information, the probability of reaching a stone with a sialenoscope is generally around 80-85%. Our success rate in removing a reached stone with the crushing method is 94% at the end of 20 years. When we recalculate these, our probability of getting results with sialendoscopy in any stone case is between 76-80%. The rates can be updated when the number, location and dimensions of the stone are learnt.
Click here to see sample cases.
Frequently Asked Questions About Salivary Gland Stone Treatment:
- Is Salivary Gland Stone Dangerous?
- How to Prevent Salivary Gland Stone?
- Is there a method other than sialendoscopy for salivary gland stone removal?
- Does the salivary gland work after stone removal?
- Does salivary gland stone recur?
- Salivary Gland Stone Removal Methods
- Is Salivary Gland Swelling Dangerous?
- What Causes Swelling of the Salivary Glands?
- Is Salivary Gland Inflammation Dangerous?
- How to Remove Salivary Gland Stone?
- What Happens If Salivary Gland Stone Is Not Treated?
- Can the salivary gland stone be felt by hand?
- How is salivary gland stone detected?